Discover the Evexia advantage Start ordering today
Take advantage of all the time and money-saving features that Evexia Diagnostics has to offer. Simply click the button below to get started.
Register Now
Serological COVID-19 spike protein antibody testing can identify individuals who have been exposed to the SARS-CoV-2 virus, regardless of symptom presentation, and quantify their personal immune response. We offer two testing options for the S-RBD antibody (spike protein receptor binding domain), the target of current COVID-19 vaccines due to the S-RBD antibodies ability to block the passage of COVID-19 to cells. The tests are optimized for pre and post vaccination testing, to deliver the information your patients need based on their individual circumstances.
When combined into a pre/post vaccination assessment, the COVID-19 Immune Response Panel and the COVID-19 Vaccine Response Screen provide clarity into not only when an individual should receive a vaccine, but the effectiveness of their body’s immune response to the inoculation.
S-RBD stands for “spike protein receptor-binding domain.” The COVID-19 S-RBD binds to the ACE2 receptor and allows the virus access to the body’s cells. Higher levels of S-RBD antibodies have been shown to block or “neutralize” the COVID-19 virus from getting into cells and causing infection.
Typically, Individuals who have recovered from a COVID-19 viral infection usually have high levels of antibodies specific to S-RBD. The “neutralizing” ability of S-RBD antibodies is why all three of the Emergency Use Authorized (EUA) vaccines target the S-RBD, although they use different methods for getting the S-RBD protein information into the body.
While human studies indicate that spike protein and nucleocapsid protein antibodies elevate in response to COVID-19 virus exposure, these antibodies are not as specific as the S-RBD antibodies for preventing COVID-19 infection (or re-infection) or for confirming post-vaccination status. After the virus infects the human body, it creates a large quantity of both “neutralizing” antibodies such as S-RBD and many nonspecific endogenous antibodies.
Although a general trend of post-infection increases in spike and nucleocapsid antibodies in association with increased S-RBD antibodies has been observed, measurement of the generalized antibodies is not always predictive of S-RBD status, particularly when the only stimulus is an S-RBD vaccine:
The COVID-19 Vaccine Response Screen measures only the antibody response to the S-RBD protein. Once the baseline immune response has been established, this test can be used post-vaccination to evaluate immune status. The average time for seroconversion has been estimated at 2-3 weeks. However, the strongest antibody responses will likely be seen after the second vaccine dose 6-8 weeks after the first inoculation.


Each test is performed using a Roche enzyme-amplified chemiluminescence platform (CLA) to detect even exceptionally small amounts of SARS-CoV-2 antibodies. The CLA technique features higher sensitivity than conventional ELISA or rapid lateral flow tests and was purposely selected based on the 30+ years of experience in immunoassay development of our laboratory partner. We are confident this process provides the most accurate results.
These tests are FDA authorized for emergency use.



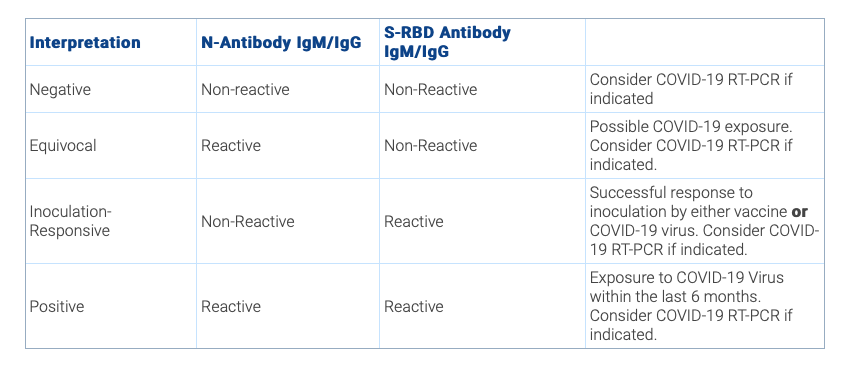
The reports are straightforward and easy to read, so you and your patient can focus on follow-up care. The reports for the COVID-19 Spike Protein Antibody tests clearly indicate if S-RBD antibodies are present and, when tested for, indicates whether IgG and IgM levels are reactive. The reports also include important information about the test.

How long does it take to get test results?
Do these tests indicate an active COVID-19 infection?
Are these tests FDA-approved?
What are the sensitivity and specificity of these tests?
Can these tests be combined with the COVID-19 Diagnostic Test?
Can these tests be used for children?
Once the specimen has been received by the lab, you can expect test results in 24-48 hours. 99% of results are available in 24 hours and 5% in 48 hours. You will be able to view the results via our online portal.
Antibody tests are not considered diagnostic for COVID-19. The COVID-19 Immune Response Panel measures IgM antibodies which can rise during an active infection.
If an individual is symptomatic or has been recently exposed to COVID-19 we suggest following up with a molecular diagnostic assay to rule out infection in these individuals.
The COVID-19 Immune Response Panel and COVID-19 Vaccination Response Screen have been FDA-authorized for emergency use.
State-of-the-art, highly sensitive chemiluminescent platforms are used to run these tests. These machines are developed and manufactured in the US and offer the most accurate IgM and IgG coronavirus antibody testing currently available.
The COVID-19 Immune Response Panel has an overall specificity of 99.8% and a sensitivity of 100% at >14 days post-infection.
Yes. Consider combining the COVID-19 antibody and diagnostic tests if:
There is evidence that this type of test is not as accurate for children. We do not recommend using these tests for children under the age of 2, or children of any age that are currently breastfeeding.

Take advantage of all the time and money-saving features that Evexia Diagnostics has to offer. Simply click the button below to get started.
Register Now